Expected early eGFR dip with subsequent renal stability after SGLT2 inhibitor initiation in CKD
21 May 2026
Share
In brief
Chronic kidney disease (CKD) continues to rise in Asia, largely driven by type 2 diabetes mellitus (T2DM), hypertension and obesity, with many patients presenting late and carrying a high burden of comorbidities.1,2 While sodium-glucose cotransporter-2 (SGLT2) inhibitors are now recommended as a cornerstone of CKD management, concerns around early renal function changes often contribute to hesitation in real-world practice.3,4 This retrospective pilot study, conducted at a secondary hospital in Malaysia, evaluated changes in renal and glycemic parameters following SGLT2 inhibitors initiation in a high-risk CKD population.2 Findings show a modest early decline in estimated glomerular filtration rate (eGFR), followed by gradual decline between 6 and 12 months, offering local reassurance on the renal safety of SGLT2 inhibitors initiation, even in multi-morbid patients.2
Background
CKD represents a growing clinical and public health challenge, particularly in regions with a high incidence of T2DM, hypertension, and obesity.1 Beyond progressive loss of kidney function, CKD is closely intertwined with cardiovascular disease, contributing substantially to morbidity, mortality, and healthcare utilization.1
In recent years, guideline-directed medical therapy for CKD has evolved toward a multi-pillar approach.5 Alongside renin-angiotensin system blockade, SGLT2 inhibitors, mineralocorticoid receptor antagonists (MRAs), and glucagon-like peptide-1 receptor agonists (GLP-1RAs) now form the therapeutic foundation of CKD management.5 Importantly, SGLT2 inhibitors occupy a unique position, serving as a core component of care in both CKD and heart failure.3,5
However, despite robust evidence from large international trials, adoption of SGLT2 inhibitors in clinical practice has historically lagged.4 Limited knowledge and cost constraints, coupled with clinician concerns regarding renal safety (particularly in older patients with multiple comorbidities) continue to influence prescribing decisions.4 Moreover, patients treated in routine practice often differ substantially from those enrolled in clinical trials, raising questions about how their findings translate to local, real-world populations.2
Against this backdrop, a pilot real-world study was conducted to evaluate renal and glycemic outcomes following SGLT2 inhibitor initiation in a Malaysian CKD cohort, which was characterized by high burden of comorbidities.2
Methodology
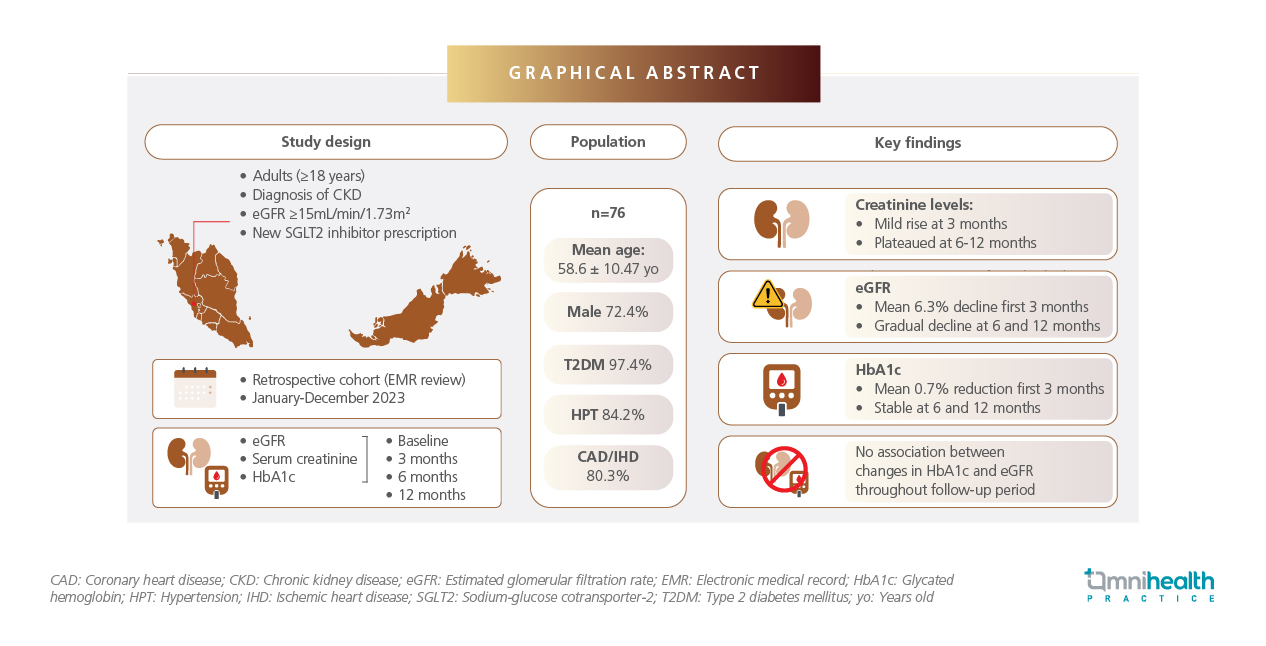
This retrospective cohort study was conducted from January to December 2023 at Hospital Shah Alam, a secondary care facility in Malaysia.2 Adult patients with established CKD who were initiated on an SGLT2 inhibitor, either empagliflozin or dapagliflozin, were identified through the hospital’s electronic medical record system from either outpatient or inpatient encounters during the study period.2 Prescription records were cross-checked with laboratory data for the baseline renal function and eligibility.2 Eligible patients were 18 years or older with an eGFR above 15mL/min/1.73m2.2 Patients with type 1 diabetes, eGFR <30mL/min/1.73m2, prior SGLT2 inhibitor use, known hypersensitivity to SGLT2 inhibitors, or those who were pregnant or breastfeeding were excluded.2
Baseline demographic and clinical characteristics, including age, sex, comorbidities, type of SGLT2 inhibitor prescribed, concomitant medications, renal profile, and glycated hemoglobin (HbA1c) at initiation, were recorded prior to therapy.2 Follow-up renal profiles and HbA1c measurements were obtained at approximately 3, 6, and 12 months post-initiation.2 The primary endpoint assessed changes in serum creatinine and eGFR following SGLT2 inhibitor initiation, while the secondary endpoint examined changes in HbA1c levels over time.2
Results
The study included 76 patients with a mean age of 58.6 years, of whom 72% were male.2 Malays comprised 73.7% of the cohort.2 Most patients had significant comorbidities, with 97.4% having T2DM, 80.3% diagnosed with ischemic or coronary artery disease, and 84.2% with hypertension.2 Spironolactone use was relatively high (31.6%), despite only about 63% receiving angiotensin-converting-enzyme (ACE) inhibitors (44.7%) or angiotensin receptor blockers (ARBs) (18.4%).2 This prescription pattern likely reflects the high burden of cardiovascular disease, particularly heart failure and ischemic heart disease in this cohort.2
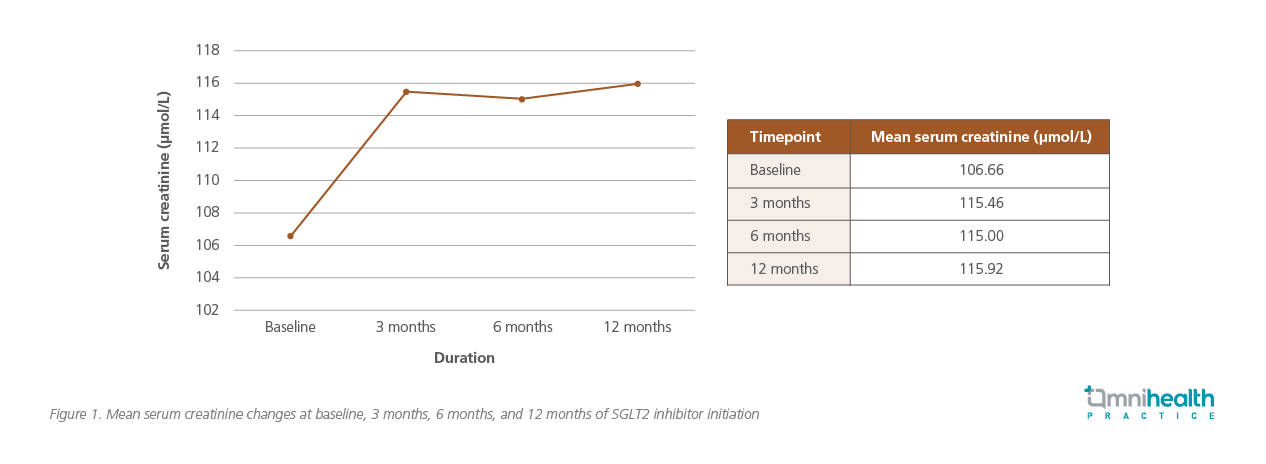
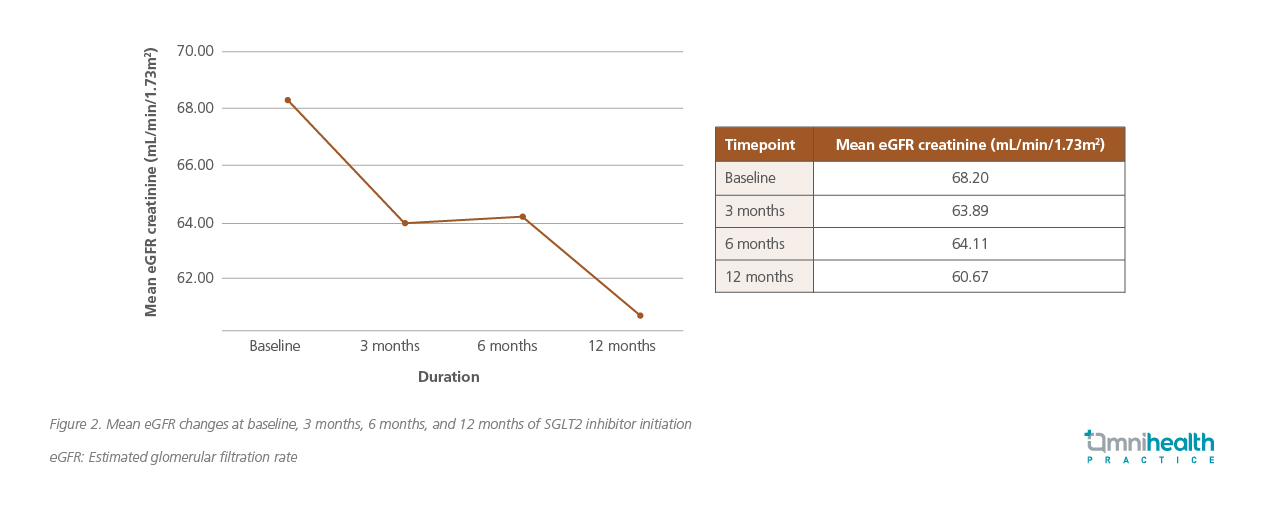
At 3 months after initiating SGLT2 inhibitor therapy, patients experienced a modest rise in serum creatinine (figure 1), reflecting the expected early hemodynamic effect of SGLT2 inhibition.2 Correspondingly, eGFR declined by 6.3% during this period.2 Between 6 and 12 months, eGFR continued to decline gradually (figure 2), while serum creatinine remained largely stable, highlighting the non-linear relationship between these two measures over time, which may be further influenced by age-related decline, comorbidities, and laboratory variability.2 Overall, mean eGFR differed significantly across all time points (p=0.001), with the largest change observed between baseline and 12 months (p=0.004).2
HbA1c improved significantly following SGLT2 inhibitor initiation, with mean values decreasing from 8.42% at baseline to 7.68% at 3 months, and remaining relatively stable at 7.78% and 7.70% at 6 and 12 months, respectively.2 This consistent glycemic response was observed despite the cohort’s substantial comorbidity burden.2 Notably, no significant association observed between changes in HbA1c and eGFR decline may be attributable to the short follow-up period, given that long-term glycemic control is more predictive of renal deterioration.2 Additionally, comorbid conditions such as hypertension and cardiovascular disease may have contributed to the observed decline in eGFR.2
Discussion
In an interview with Omnihealth Practice, Dr. Bay emphasized that the early decline in eGFR observed in this study reflects a well-recognized hemodynamic effect of SGLT2 inhibition. By modulating tubuloglomerular feedback, SGLT2 inhibitors reduce intraglomerular pressure, leading to an initial dip in eGFR—typically within the first 2-4 weeks of therapy.6 “From a mechanistic standpoint, this early change is expected and usually does not exceed 10%,” Dr Bay explained.
In day-to-day practice, this highlights the importance of setting appropriate expectations when initiating SGLT2 inhibitors.7 Patients should be counselled regarding potential increased in urine output during the early phase of treatment and advised on increasing fluid intake.7 They should also be reassured that transient changes in renal indices are anticipated.7 Dr. Bay also noted that an early follow-up, particularly within the first couple of weeks of SGLT2 inhibitor initiation can be helpful to assess volume status, blood pressure, and patient tolerance, especially in primary care settings.
In this high‑risk cohort with significant comorbidities, the modest early decline in eGFR that remained below the 10% threshold defined by the Kidney Disease: Improving Global Outcomes (KDIGO) 2024 guideline supports the renal safety of SGLT2 inhibitor initiation.2 The more pronounced decline observed in subsequent months likely reflects underlying disease progression rather than a treatment effect.2 However, in the absence of a control group in this study, it cannot be determined whether this trajectory differs from the expected natural course of CKD.2
More pronounced renal protective effects of SGLT2 inhibitors have been demonstrated in real-world data from a large retrospective cohort in China.7 In this study of 944 patients with CKD and T2DM followed for 17-19 months, SGLT2 inhibitor use was associated with a significantly slower rate of eGFR decline compared with other glucose-lowering drug (oGLD) therapies.7 The mean annual eGFR decline was 0.02mL/min/1.73m2 (95% CI: −2.9 to 3.4) in the SGLT2 inhibitor group vs. 4.96mL/min/1.73m2 (95% CI: 2.33-7.63) in the oGLD group, yielding a between-group difference of 4.94mL/min/1.73m2 per year (95% CI: 4.73-5.15; p<0.001) in favor of SGLT2 inhibition.7 These findings are consistent with the landmark DAPA-CKD trial, which demonstrated sustained renal protection with SGLT2 inhibition, irrespective of diabetes status.2
The findings also reinforce the overall renal safety of SGLT2 inhibitors, even among older and multi-morbid patients.2 He mentioned, “Our patients carry multiple comorbidities, and often present late. Yet, even in this high-risk group, SGLT2 inhibitors demonstrated predictable and manageable renal changes.” Common adverse effects, such as dehydration and urinary tract infections, can generally be mitigated through patient education and monitoring.7 Rare but recognized complications, as Dr. Bay noted, include euglycemic diabetic ketoacidosis, underscoring the importance of sick-day counselling and temporary discontinuation of SGLT2 inhibitors during acute illness or prior to major surgery.
Despite strong evidence supporting the renal benefits and safety of SGLT2 inhibitors, real-world utilization remains suboptimal.8 Local prescribing data from Malaysia (2021–2022) indicate a gap between evidence-based recommendations and routine clinical practice among eligible patients.8 Addressing this gap may allow more patients to benefit from long-term renal protection.8 As Dr. Bay noted, “Hopefully, as we move toward 2026, the use of SGLT2 inhibitors will increase, allowing more patients to benefit.”
Dr. Bay also cautioned on several limitations that should be considered when interpreting these findings. The retrospective design precludes causal inference, and key confounders, such as blood pressure control, heart failure severity, and the contribution of other therapeutic pillars, were not fully accounted for. Additionally, access constraints influenced patient selection, potentially biasing the cohort toward those at higher risk of disease progression. He further calls for larger, prospective real-world studies incorporating broader patient populations and multiple treatment pillars to better reflect the complexity of CKD management in routine practice.
Conclusion
Taken together, this pilot real-world study provides clinically relevant reassurance that SGLT2 inhibitors can be safely initiated in high-risk patients with CKD, with early changes in renal function that are predictable, modest, and stabilize over time.2 These findings help contextualize early eGFR changes and support earlier and more confident use of SGLT2 inhibitors as part of comprehensive CKD care.2 Dr. Bay further emphasized that the clinical impact of SGLT2 inhibitors is greatest when they are introduced early rather than reserved for advanced disease. “If we want to truly delay CKD progression, SGLT2 inhibitors should be initiated earlier, before patients reach the end of the disease spectrum.”
References
- Makmun A, et al. The burden of chronic kidney disease in Asia region: a review of the evidence, current challenges, and future directions. Kidney Res Clin Pract. 2024;44(3):411.
- Bay SS, et al. The impact of initiating SGLT2 inhibitors on eGFR: a pilot study at a secondary hospital in Malaysia. BMC Res Notes. 2025. In Press.
- Stevens PE, et al. KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2024;105(4):S117-314.
- Ng NM, et al. Factors affecting prescription of sodium-glucose co-transporter 2 inhibitors in patients with type 2 diabetes mellitus with established cardiovascular disease/chronic kidney disease in Hong Kong: a qualitative study. BMC Prim Care. 2022;23(1):317.
- Agarwal R, et al. The foundation and the four pillars of treatment for cardiorenal protection in people with chronic kidney disease and type 2 diabetes. Nephrol Dial Transplant. 2023;38(2):253-7.
- An HJ, et al. Impact of age on eGFR dynamics following sodium-glucose cotransporter 2 inhibitor therapy: A real-world study. Diabetes Res Clin Pract. 2024;214:111796.
- Xiao X, et al. Kidney outcomes associated with SGLT2 inhibitors compared to other glucose-lowering drugs: a real-world study from China. Front Pharmacol. 2024;15:1468435.
- Lim LL, et al. Real-world evaluation of care for type 2 diabetes in Malaysia: A cross-sectional analysis of the treatment adherence to guideline evaluation in type 2 diabetes (TARGET-T2D) study. PLoS One. 2024;19(1):e0296298.




 – Dr. Fariz_KV_250904")